If you want fat loss without GLP-1 drugs, you still have powerful, evidence-based tools. By combining growth hormone (GH) secretagogues that promote lipolysis, targeted nutrient support, and hormone optimization (including thyroid), you can reduce visceral fat, protect lean mass, and improve metabolic health, all while staying within the bounds of human clinical evidence1.
At Vita Bella, we believe lasting weight loss isn’t about shortcuts; it's about science, balance, and personalization. If GLP-1s aren’t right for you, there are still powerful, proven options to ignite fat loss naturally. Our experts combine peptide therapy, hormone optimization, and targeted nutrition to help your body burn fat efficiently. Experience precision, not guesswork, your transformation starts with Vita Bella.
Why look beyond GLP-1?
GLP-1s help many people, yet some prefer alternatives due to cost, access, or tolerability. Fortunately, human studies2 show that other pathways can drive fat loss, especially visceral adipose tissue (VAT), with minimal effects on subcutaneous fat, which strongly influences metabolic risk when interventions are carefully chosen and monitored.
What are the GH secretagogues that support lipolysis?
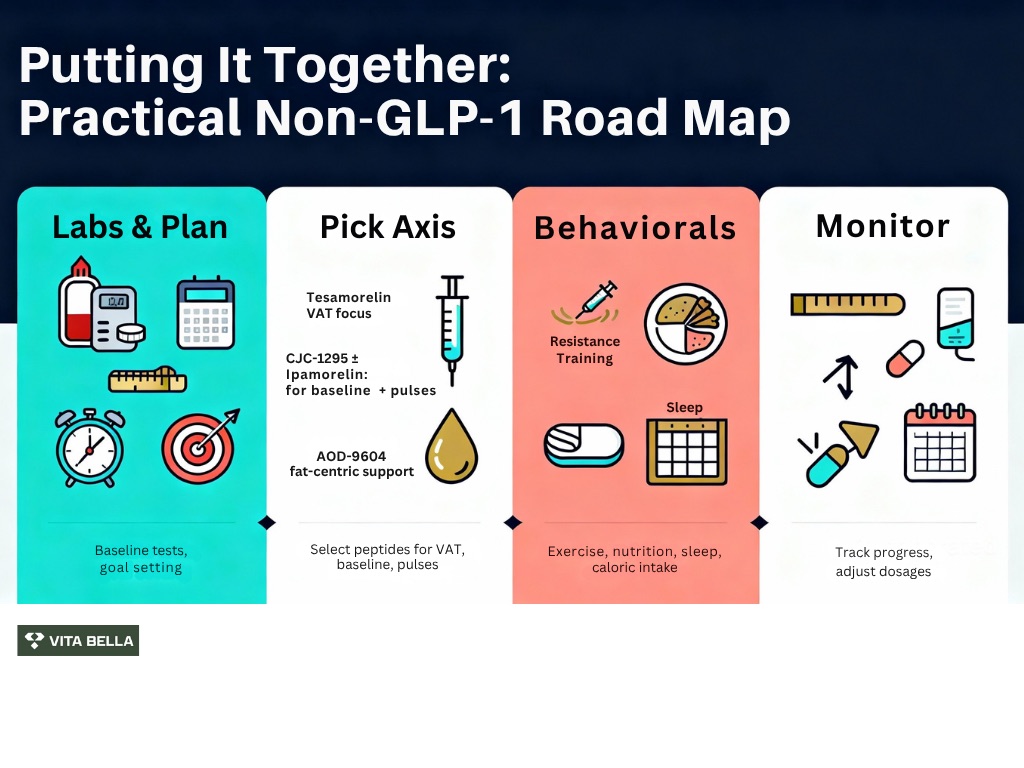
Growth hormone (GH) secretagogues are compounds that stimulate the release of GH, which plays a vital role in lipolysis (fat breakdown). Some of the most popular GH secretagogues that support lipolysis include peptides such as CJC-1295, Ipamorelin, and Tesamorelin. Let’s look into how they can be incorporated into a comprehensive fat-loss strategy:
1- Tesamorelin: targeted VAT reduction with RCT data
Tesamorelin, a stabilized GHRH analog, consistently reduces visceral adipose tissue (VAT) in adults with central adiposity. In a randomized, double-blind, placebo-controlled trial2, daily intake of tesamorelin reduced VAT and also lowered liver fat, highlighting benefits beyond the beltline; results were clinically meaningful and supported metabolic improvements.
2- CJC-1295 (+/- ipamorelin): sustained baseline + programmable pulses
CJC-1295 extends GHRH signaling for days, creating a durable rise in GH/IGF-1 that many use to support steadier recovery and body composition. As per research3, in healthy adults, subcutaneous CJC-1295 produced sustained, dose-dependent increases in GH and IGF-1 and was well tolerated, a strong platform when you want less frequent dosing.
Ipamorelin can layer brief, titratable GH pulses on top of that baseline. In healthy volunteers, dose-escalation human PK/PD modeling mapped predictable GH release across infusion rates, enabling individualized pulse timing alongside training or evening recovery. According to a study4, a single GH release episode with a peak at 0.67 hours and an exponential decline to an insignificant GH concentration was observed in the time course of GH stimulation by ipamorelin across all dosages.
Why can GH support help with fat loss?
GH physiology directly favors fat use: in human studies5, increased pulsatile GH secretion stimulates lipolysis, mobilizing fatty acids while helping preserve lean tissue, a valuable combination during calorie restriction or recomposition programs. Practically, this means better fat-mass targeting without the need to chase extreme calorie cuts.
Is AOD-9604 effective for supporting lipolysis without promoting muscle gain?
AOD-9604 (a fragment of the hGH 177–191 sequence) has been evaluated in multiple human trials6 with a favorable safety profile and no increase in IGF-1, an advantage for those who want fat-focused effects without anabolic signaling. These data support its role as a non-GLP-1 option aimed at fat metabolism support.
Are "Bio-Boost" MIC injections (lipotropics) effective as an adjunct treatment?
Methionine-Inositol-Choline (often with B12) is used clinically to support energy metabolism and behavior change during fat-loss programs. While MIC is not a stand-alone pharmacologic weight-loss therapy, many patients find that improved energy and adherence make diet, training, and recovery more consistent, amplifying results alongside the options above.
Should other hormones be optimized first before starting treatment?
Optimizing hormone levels before starting treatment is crucial to ensuring the effectiveness of any therapeutic regimen. Ensuring there are no uphill battles of unblanced hormones such as thyroid, cortisol, and insulin can help improve metabolic function, enhance energy levels, and support overall health. Hormone optimization creates a stable foundation, which can make treatments more effective and reduce potential side effects. Here are some key considerations to keep in mind:
1- Check thyroid, a small gland, has a significant impact.
Unrecognized hypothyroidism slows metabolic rate and frustrates fat loss. Treating overt hypothyroidism with levothyroxine or other therapies improves metabolic parameters and can reduce weight, particularly water and fat mass, thereby restoring a favorable environment for sustainable fat loss with or without adjuncts. Screening TSH/free T4 (and treating when indicated) is a high-leverage step.
2- Align testosterone, sleep, and nutrition.
Balanced testosterone, deep sleep, and adequate protein help preserve lean mass while you lose fat. Moreover, resistance training synergizes with GH-axis support to prioritize fat over muscle in a caloric deficit. This “protect the engine while burning fuel” approach sustains metabolic rate and keeps results durable.
Move Beyond GLP-1, achieve Lasting Results with Vita Bella.
You’re tired of relying on injections that drain your wallet and disrupt your rhythm. GLP-1s may suppress appetite, but they don’t fix your metabolism. The real issue isn’t lack of willpower; it’s hormonal imbalance and sluggish fat signaling. Your body deserves a more innovative, sustainable solution.
At Vita Bella, we optimize your metabolism naturally, no GLP-1 required. Through peptide therapy, thyroid balance, and hormone precision, we awaken your body’s own fat-burning pathways. Our approach reshapes your metabolism from the inside out. Rediscover control, confidence, and balance the Vita Bella way.
FAQs
Can GH secretagogues really help with fat loss?
Yes, human studies show that GH secretagogues such as tesamorelin, CJC-1295, and ipamorelin stimulate lipolysis, the breakdown of stored fat, while preserving lean muscle. These peptides work by increasing natural growth hormone pulses, which mobilize fatty acids for energy. Regular monitoring and personalized dosing make this approach both safe and effective.
Is AOD-9604 a safe weight-loss option for women?
Clinical data demonstrate that AOD-9604, a modified GH fragment, can enhance fat metabolism without elevating IGF-1 or increasing muscle mass, making it ideal for women seeking targeted fat reduction. It supports lipolysis without androgenic effects, offering a gentler, non-stimulant path to fat loss and improved balance in body composition.
Should I check my thyroid before starting any fat-loss therapy?
Yes, thyroid hormones directly regulate metabolic rate and fat utilization. Even mild hypothyroidism can slow fat loss and mimic weight-loss resistance. A complete thyroid panel (TSH, free T4, and free T3) helps identify hidden imbalances. Correcting and normalizing thyroid function can accelerate fat metabolism and optimize the effects of GH secretagogues or other interventions.
Do I need injections like GLP-1 drugs to lose weight effectively?
No, sustainable fat loss can be achieved through hormonal optimization, improved nutrition, and metabolic enhancers like GH secretagogues or MIC “Bio-Boost” injections. These alternatives stimulate natural fat burning, support energy production, and preserve lean mass, providing a more balanced, long-term solution without the gastrointestinal side effects seen with GLP-1s.
References:
Falutz, J., Allas, S., Blot, K., Potvin, D., Kotler, D., Somero, M., Berger, D., Brown, S., Richmond, G., Fessel, J., Turner, R., & Grinspoon, S. (2007). Metabolic effects of a growth hormone–releasing factor in patients with HIV. The New England Journal of Medicine, 357(23), 2359–2370. https://doi.org/10.1056/NEJMoa072375
Stanley, T. L., Feldpausch, M. N., Oh, J., Branch, K. L., Lee, H., Torriani, M., & Grinspoon, S. K. (2014). Effect of Tesamorelin on visceral fat and liver fat in HIV‑infected patients with abdominal fat accumulation: A randomized clinical trial. JAMA, 312(4), 380–389. https://doi.org/10.1001/jama.2014.8334
Teichman, S. L., Neale, A., Lawrence, B., Gagnon, C., Castaigne, J.-P., & Frohman, L. A. (2006). Prolonged stimulation of growth hormone (GH) and insulin‑like growth factor I secretion by CJC‑1295, a long‑acting analog of GH‑releasing hormone, in healthy adults. The Journal of Clinical Endocrinology & Metabolism, 91(3), 799–805. https://doi.org/10.1210/jc.2005‑1536
Gobburu, J. V. S., Agersø, H., Jusko, W. J., & Ynddal, L. (1999). Pharmacokinetic‑pharmacodynamic modeling of ipamorelin, a growth hormone releasing peptide, in human volunteers. Pharmaceutical Research, 16(9), 1412‑1416. https://doi.org/10.1023/A:1018955126402
Goldenberg, N., Horowitz, J. F., Gorgey, A., Sakharova, A., & Barkan, A. L. (2022). Role of pulsatile growth hormone (GH) secretion in the regulation of lipolysis in fasting humans. Clinical Diabetes and Endocrinology, 8(1), 1–8. https://doi.org/10.1186/s40842-022-00137-y
Stier, H., Vos, E., & Kenley, D. (2013). Safety and tolerability of the hexadecapeptide AOD9604 in humans. Journal of Endocrinology & Metabolism, 3(1‑2), 7–15. https://doi.org/10.4021/jem157w